









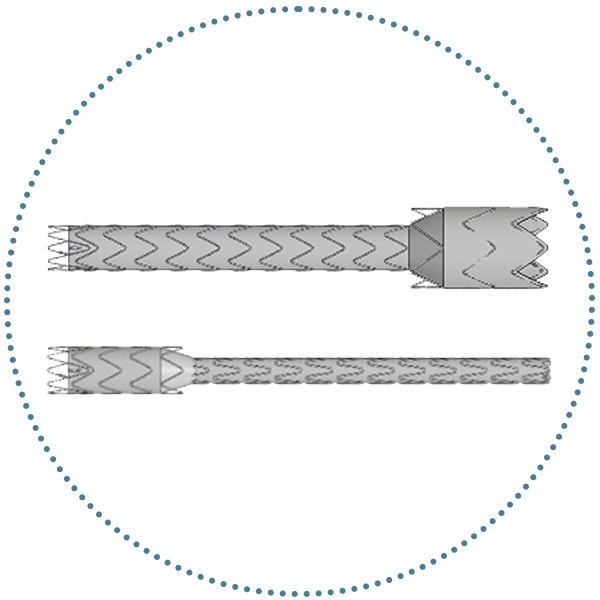






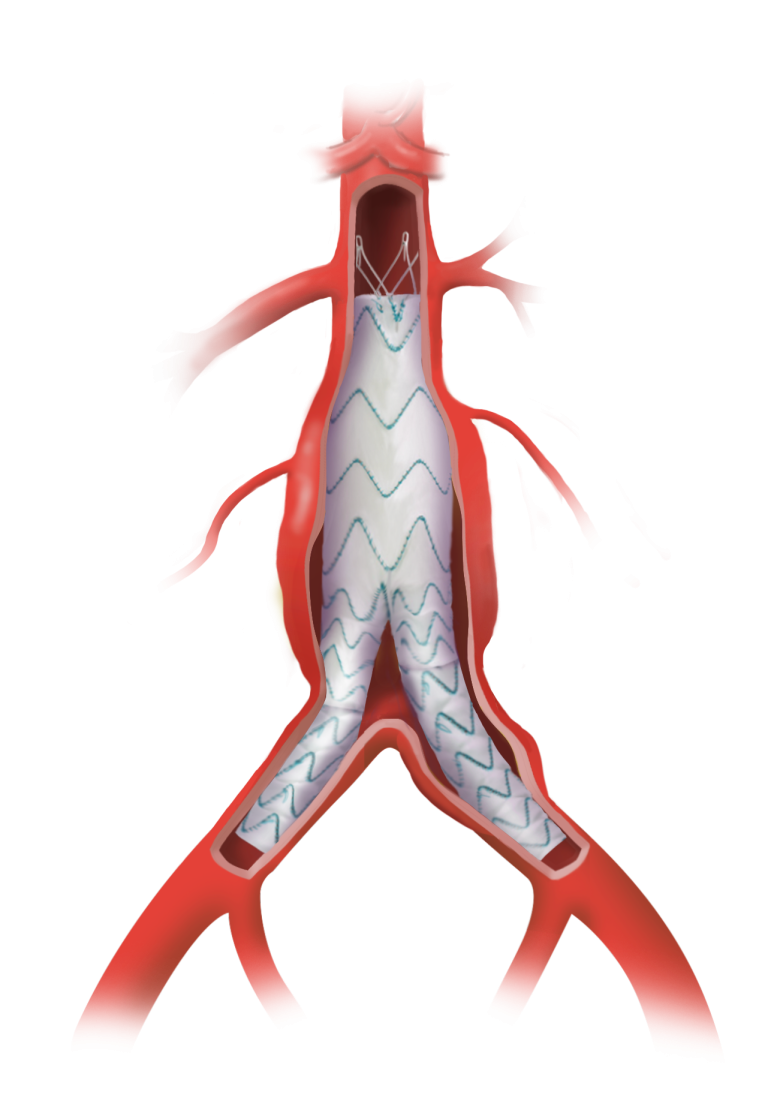
Discover how the TREO® Abdominal Stent-graft System supports in achieving EVAR success with sac regression.
Click to learn more

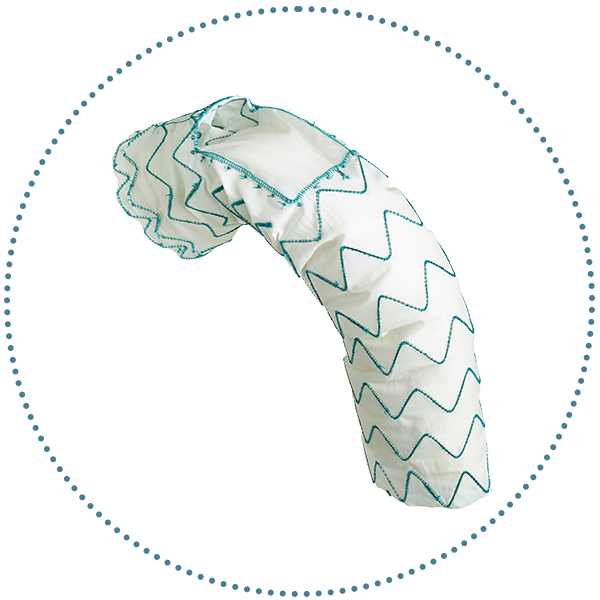
Discover how the Relay®Pro Thoracic Stent-graft System delivers proven neurological results.
Click to learn more
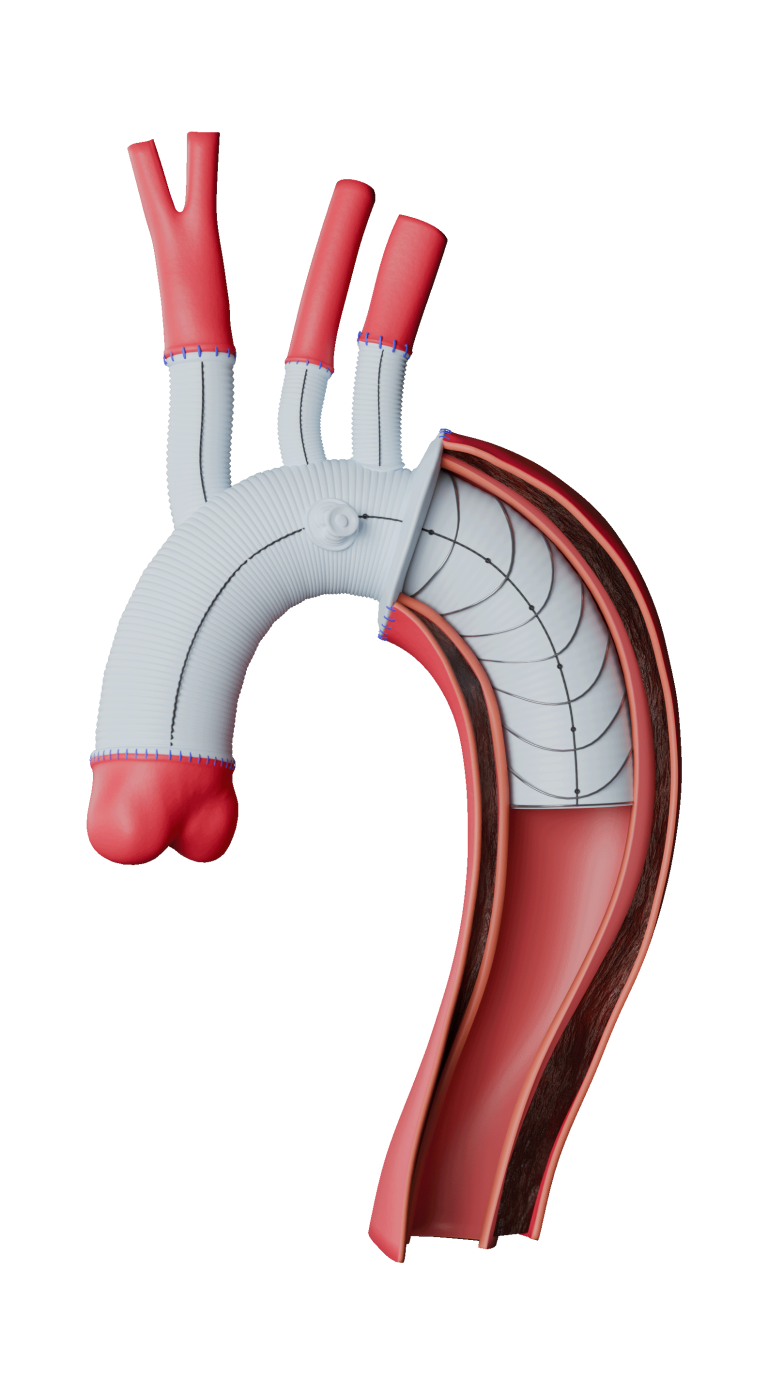
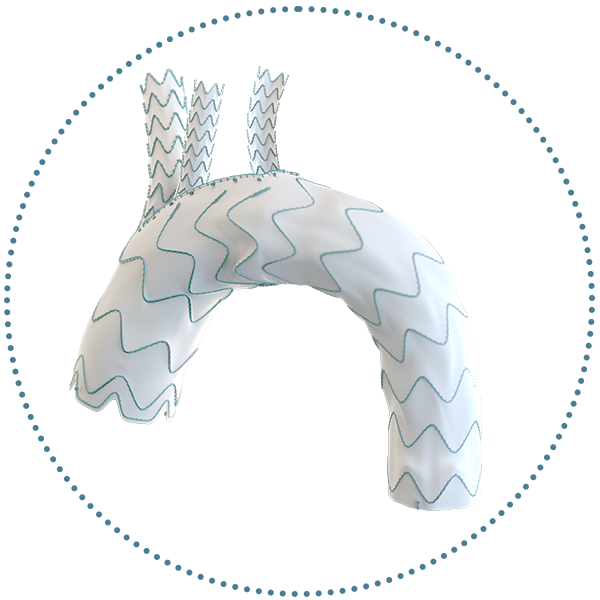
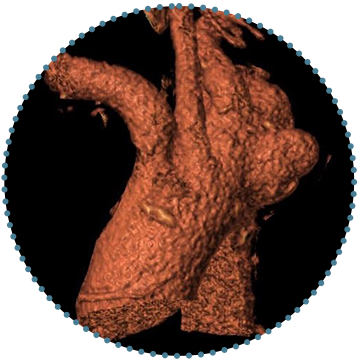
Discover Remodelling and Aneurysmal Regression with Thoraflex™ Hybrid
Click to learn more